CT Brain Stroke: A Complete Diagnostic Guide
Every minute that passes during a stroke, approximately 1.9 million neurons are irreversibly destroyed. This stark clinical reality underscores why CT imaging remains the single most important tool in the acute management of stroke — it is fast, widely available, and provides the critical information needed to make life-saving treatment decisions within the narrow therapeutic window of a few hours.
Why CT is the First-Line Imaging Modality for Stroke
When a patient arrives at the emergency department with sudden neurological deficits, the immediate clinical question is: is this ischemic or hemorrhagic? This distinction fundamentally determines treatment — thrombolytic therapy (tPA) is lifesaving in ischemic stroke but catastrophically harmful in hemorrhagic stroke. Non-contrast CT (NCCT) of the brain answers this question within minutes, making it the universal first step in the stroke protocol.
CT's advantages in the acute setting include near-universal availability, rapid acquisition (under two minutes), and its unmatched ability to detect acute hemorrhage, which appears as a hyperdense (bright white) region on unenhanced scans — a finding that MRI can actually miss in the hyperacute phase due to the complexity of hemoglobin oxidation states.
Understanding Normal Brain CT Anatomy
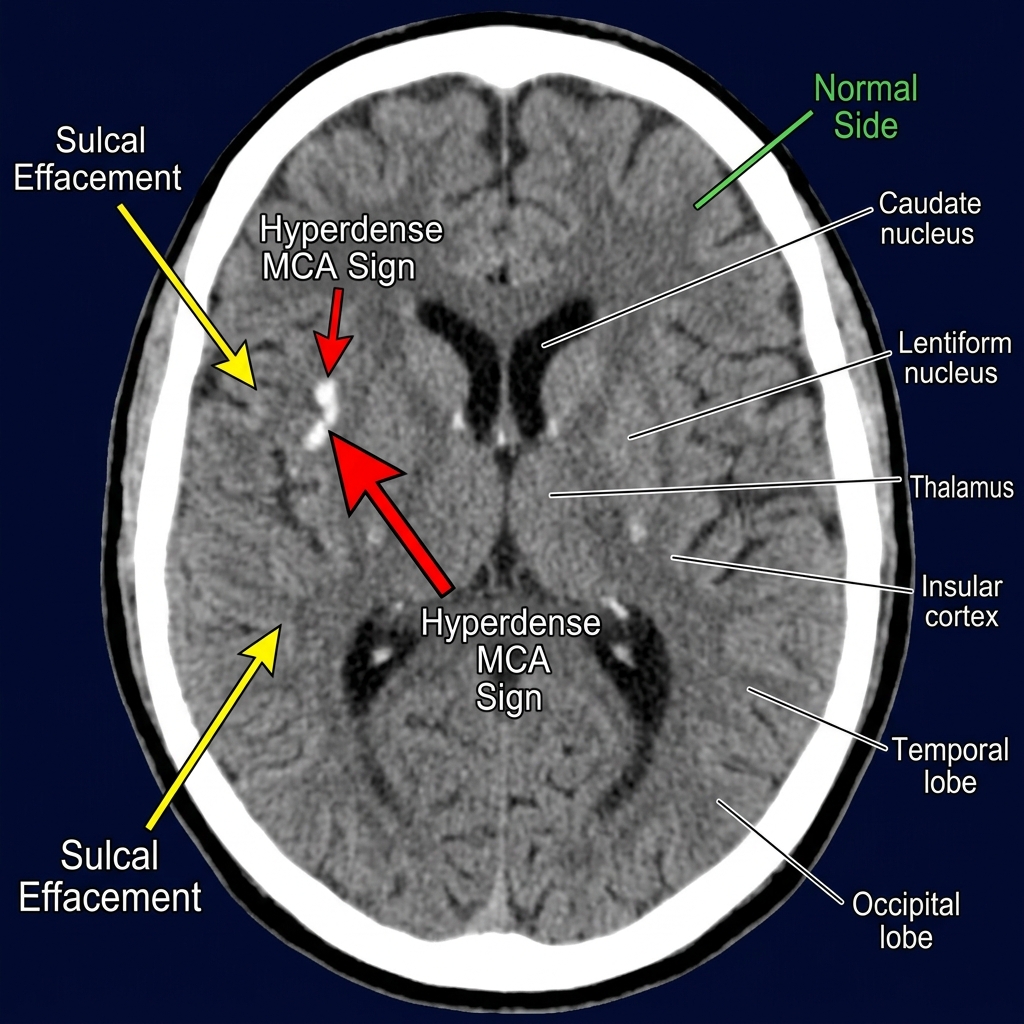
Accurate stroke diagnosis on CT requires a thorough understanding of the normal appearance. The brain parenchyma is assessed on a brain window (W:80, L:40), where gray matter appears slightly more hyperdense than white matter. The basal ganglia, thalami, insular cortex, and internal capsule are key structures to evaluate systematically. Symmetry is the radiologist's most powerful tool — any asymmetry in density, sulcal pattern, or grey-white differentiation demands careful attention.
Early CT Signs of Ischemic Stroke
Many radiologists and emergency physicians are taught that CT is "negative" in early ischemic stroke, but this is a dangerous oversimplification. Within the first 3–6 hours, several subtle but critical signs may be present.
1. The Hyperdense MCA Sign
The hyperdense middle cerebral artery (MCA) sign is one of the earliest and most specific findings in ischemic stroke. It appears as an abnormally bright (hyperdense) MCA compared to the contralateral side, reflecting a fresh thrombus within the vessel. When the clot extends to the M1 segment bifurcation, a dot sign may be seen in the Sylvian fissure. This sign has a specificity of approximately 90–95% for acute large vessel occlusion and is a strong predictor of poor outcome without intervention.
2. Loss of the Insular Ribbon Sign
The insular cortex — the deep strip of gray matter that lines the Sylvian fissure — is one of the most sensitive areas to ischemia due to its position at the terminal supply of the MCA with limited collateral flow. Loss of the normal gray-white distinction in this region, where the insular ribbon appears smudged or indistinguishable from the adjacent white matter, is an early sign of MCA territory ischemia. This subtle finding can be present within 1–2 hours of stroke onset.
3. Sulcal Effacement and Cortical Swelling
Cytotoxic edema — the early stage of ischemic swelling at the cellular level — causes subtle loss of sulcal markings over the affected cortex. The gyri appear swollen and the sulci are compressed or absent compared to the normal contralateral hemisphere. This finding, combined with subtle hypoattenuation of affected cortex, often precedes the dramatic infarct changes seen at 24–48 hours.
4. The ASPECTS Scoring System
The Alberta Stroke Program Early CT Score (ASPECTS) is a standardized, reproducible 10-point scoring system that evaluates early ischemic changes in the MCA territory. Ten regions are assessed: M1–M6 (six cortical regions) plus the internal capsule (IC), basal ganglia (BG), caudate (C), and lentiform nucleus (L). Each region showing early ischemia subtracts one point from the base score of 10. An ASPECTS score ≤6 is associated with poor outcome and guides eligibility for endovascular thrombectomy in many international guidelines.
CT Findings of Hemorrhagic Stroke
Acute intracerebral hemorrhage (ICH) is unmistakable on CT — it appears as a well-defined, markedly hyperdense (70–90 HU) collection within the brain parenchyma. The location of a hemorrhage provides critical clues to its etiology:
- Basal ganglia and thalamus: Hypertensive hemorrhage — the most common cause of deep ICH in patients over 50 with poorly controlled blood pressure
- Lobar (cortical) location: Consider cerebral amyloid angiopathy (especially in elderly patients) or an underlying lesion such as a tumor or AVM
- Cerebellar hemorrhage: A surgical emergency — can cause rapid deterioration from brainstem compression
- Pontine hemorrhage: Often catastrophic, strongly associated with chronic hypertension
Surrounding the hematoma, a rim of hypoattenuation develops and expands over the first 24–72 hours as vasogenic edema accumulates. Hematoma expansion — defined as greater than 33% volume growth or greater than 6 mL absolute growth — occurs in approximately 30–40% of patients within the first 24 hours and is a major predictor of neurological deterioration. The spot sign on CT angiography — a focus of contrast enhancement within the hematoma — predicts hematoma expansion with high specificity.
CT Angiography (CTA) in Acute Stroke
CTA of the head and neck is now a standard component of the modern stroke CT protocol. It provides:
- Direct visualization of the site of large vessel occlusion (LVO) — critical for endovascular treatment eligibility
- Evaluation of the cervical carotid and vertebral arteries for dissection, stenosis, or atherosclerotic disease
- Detection of tandem lesions (combined intracranial and extracranial occlusions)
- Assessment of collateral circulation — robust collaterals correlate with better outcomes and wider treatment windows
CT Perfusion (CTP): Mapping the Ischemic Penumbra
CT perfusion adds dynamic functional information that anatomical imaging cannot provide. By tracking an iodinated contrast bolus through the brain, CTP generates parametric maps of: Cerebral Blood Flow (CBF) — reduced in ischemic tissue; Cerebral Blood Volume (CBV) — critically reduced in the irreversibly infarcted core; and Mean Transit Time (MTT) and Time to Peak (Tmax) — prolonged in the at-risk penumbra.
The mismatch between the ischemic core (low CBV, Tmax greater than 6 seconds) and the penumbra represents salvageable brain tissue. Automated software platforms such as RAPID and OLEA now provide standardized outputs that directly guide eligibility for mechanical thrombectomy in the extended therapeutic window — up to 24 hours in selected patients, as demonstrated by the landmark DAWN and DEFUSE 3 clinical trials.
Treatment Implications of CT Findings
The CT report in acute stroke must directly address the clinical question: is this patient eligible for treatment? Key findings to document include: presence or absence of hemorrhage, ASPECTS score, site of vessel occlusion on CTA, presence of the spot sign in hemorrhagic cases, and the perfusion mismatch profile. A structured, time-sensitive report using standardized templates significantly improves the speed and accuracy of clinical decision-making in this time-critical emergency, where every minute of delay translates directly into greater neuronal loss.
Important Pitfalls and Limitations
Several important pitfalls must be recognized. Posterior fossa (cerebellar and brainstem) infarcts are notoriously difficult to detect on CT due to beam-hardening artifact from the surrounding dense bone. Small cortical infarcts and lacunar infarcts in the acute phase may be invisible on CT, making MRI with diffusion-weighted imaging (DWI) the superior modality when posterior circulation stroke is suspected clinically. Furthermore, early ischemic changes are subtle — approximately 50% of early strokes may appear entirely normal to inexperienced observers — making systematic review protocols and dual-read practices essential quality assurance measures in busy emergency radiology environments.