CT Abdomen: Diagnosing Acute Appendicitis
Acute appendicitis is the most common abdominal surgical emergency, with a lifetime risk of approximately 7–8%, affecting millions of patients globally each year. While the clinical diagnosis based on migratory right iliac fossa pain, fever, nausea, anorexia, and an elevated white cell count may be straightforward in classic presentations, up to 30% of cases present atypically — particularly in children, the elderly, pregnant women, and patients with retrocecal appendix anatomy. CT of the abdomen and pelvis has become the gold standard diagnostic tool for equivocal appendicitis, offering sensitivity of 94–100% and specificity of 91–99% that directly translates into reduced negative appendectomy rates and earlier identification of life-threatening complications.
CT Protocol for Appendicitis Evaluation
Several CT protocols are employed depending on institution, patient population, and clinical context:
- CT Abdomen and Pelvis with IV Contrast (Portal Venous Phase): The most widely used protocol, providing excellent soft tissue contrast to visualize the appendix and periappendiceal structures. IV contrast significantly improves delineation of the appendiceal wall enhancement pattern and surrounding mesenteric inflammatory change
- CT without IV Contrast: Appropriate in patients with renal impairment or contrast allergy. Sensitivity is marginally lower but remains clinically adequate when combined with strong clinical suspicion. An appendicolith is readily identified without contrast
- Low-Dose CT (LDCT): Increasingly adopted for pediatric patients and young adults to reduce radiation exposure, with multiple studies demonstrating non-inferior diagnostic accuracy for uncomplicated appendicitis compared to standard-dose CT
Normal Appendix: Anatomy and CT Appearance
Identifying the normal appendix is the critical first step. The appendix arises from the cecal tip, at the confluence of the three taeniae coli, and normally measures less than 6 mm in outer-to-outer diameter. It has a thin, enhancing wall (≤2 mm) with a narrow lumen that may contain gas, fluid, or a small amount of fecal material. Periappendiceal fat should appear completely clean with no inflammatory stranding. The appendiceal location is highly variable: retrocecal (65% of patients), pelvic, preileal, or paracolic positions are all normal anatomical variants that can dramatically alter the clinical presentation and CT search pattern.
Classic CT Findings of Acute Appendicitis
Definitive CT diagnosis of appendicitis rests on identifying a distended, non-compressible appendix with associated inflammatory changes in the surrounding tissues.
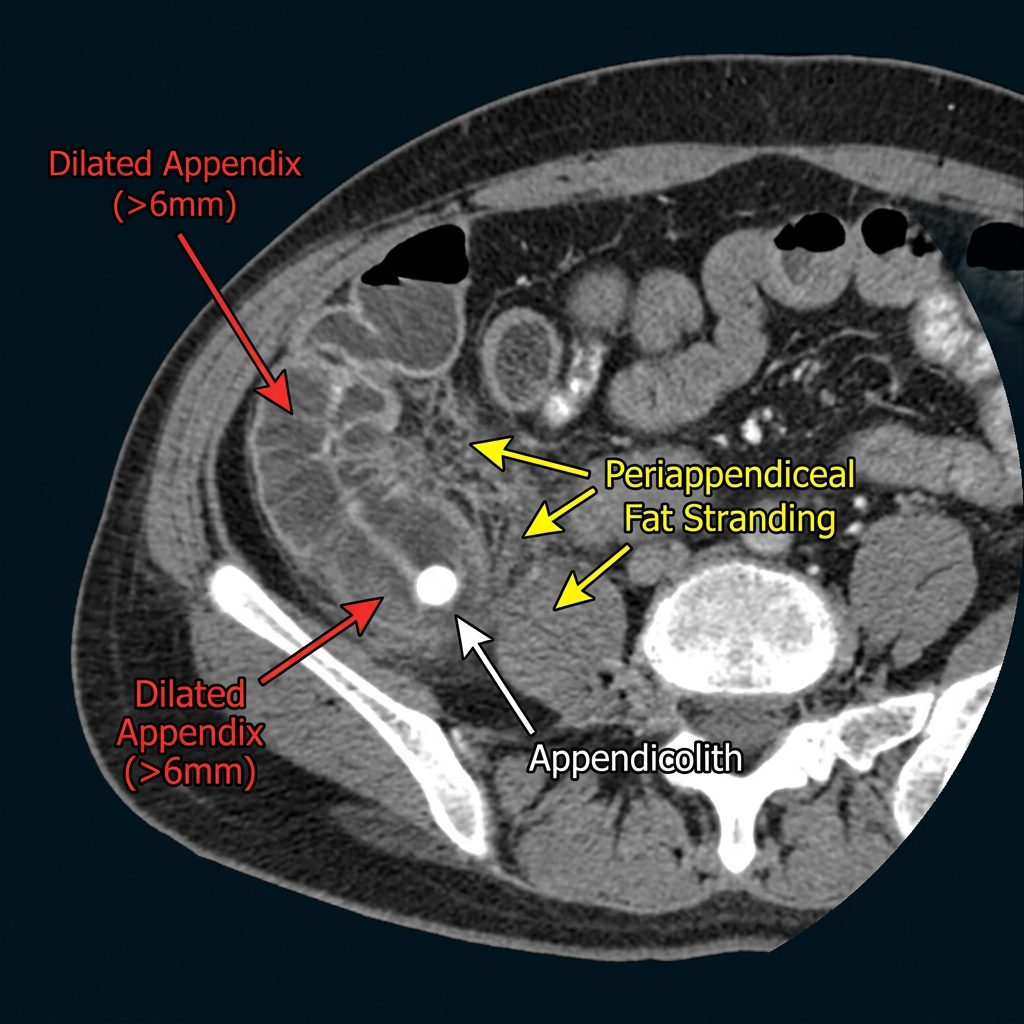
Appendiceal Dilatation
An outer-to-outer diameter greater than 6 mm is the primary diagnostic criterion for appendicitis on CT. Diameters in the 6–10 mm range are diagnostic when combined with wall thickening and periappendiceal inflammatory changes. Diameters greater than 10 mm indicate severe distension and substantially increase the probability of perforation. The appendiceal lumen is typically filled with fluid or pus, with absent intraluminal gas — a collapsed, gas-containing appendix effectively excludes acute appendicitis.
Appendiceal Wall Thickening and Enhancement Pattern
Acute appendicitis causes circumferential wall thickening greater than 2–3 mm and avid mucosal enhancement on post-contrast CT. The inner mucosal layer appears bright (hyperenhancing), reflecting acute hyperemia and inflammation. Importantly, loss of this stratified enhancement pattern — with homogeneous, low-density, non-enhancing wall thickening — suggests gangrenous appendicitis, a precursor to perforation that requires urgent surgical intervention.
Periappendiceal Fat Stranding
Periappendiceal fat stranding is present in virtually all CT-diagnosed cases of appendicitis. It appears as increased density and haziness in the mesoappendix and adjacent pericecal fat, reflecting edema, lymphatic obstruction, and inflammatory exudate from the inflamed appendiceal wall. The extent of fat stranding correlates with disease severity — contained local stranding suggests uncomplicated appendicitis, while stranding extending into the pelvis or paracolic gutters indicates spreading infection and impending or actual perforation.
Appendicolith
An appendicolith (fecalith) is a calcified concretion within the appendiceal lumen, visible in approximately 25–30% of appendicitis cases on CT. Its presence when associated with appendiceal inflammation significantly increases diagnostic specificity. An isolated appendicolith without surrounding inflammatory changes may be an incidental finding of uncertain significance. However, a free-floating appendicolith in the peritoneal cavity — seen after perforation — is pathognomonic and represents a surgical emergency.
Free Periappendiceal Fluid
A small amount of periappendiceal free fluid is common in non-perforated appendicitis and does not alone indicate perforation. Fluid that extends beyond the immediate periappendiceal region — into the pelvis, bilateral paracolic gutters, or between bowel loops — is strongly concerning for perforation with peritoneal spillage and should be urgently communicated to the surgical team.
Complicated Appendicitis: Recognizing the Full Spectrum
Gangrenous Appendicitis
Gangrenous appendicitis represents transmural infarction of the appendiceal wall due to vascular occlusion from severe intraluminal pressure and inflammation. CT findings include: absent or asymmetric mural enhancement, intramural gas (pneumatosis appendicis), and disruption of the normal layered wall structure. This is a pre-perforation state requiring emergency surgery. Radiologists should communicate this finding with urgency even in the absence of overt perforation.
Perforated Appendicitis
CT is highly sensitive for perforation detection. Pathognomonic and strongly suggestive features include: extraluminal gas (free air in the periappendiceal region or pelvis — pathognomonic when present), a visible appendiceal wall defect on thin-section imaging, and a periappendiceal abscess appearing as a rim-enhancing, thick-walled fluid collection adjacent to the cecal tip. A free-floating appendicolith in the peritoneum is essentially diagnostic of perforation with failed containment.
Periappendiceal Phlegmon and Abscess
A phlegmon appears as an ill-defined, heterogeneous inflammatory soft-tissue mass in the right iliac fossa, without a discrete fluid-filled cavity. An abscess, by contrast, is a rim-enhancing collection with a defined wall, often containing air-fluid levels. When a mature abscess is present, surgical management may initially be deferred in favor of CT-guided percutaneous drainage followed by a delayed interval appendectomy — an approach that reduces operative morbidity in the setting of severe local inflammation.
Right Iliac Fossa Differential Diagnosis
When the appendix appears normal or cannot be confidently visualized on CT, a systematic differential diagnosis of the right iliac fossa must be explored:
- In reproductive-age women: Ovarian cyst, ovarian torsion, ectopic pregnancy (urgent — check beta-hCG), endometriosis, pelvic inflammatory disease (PID), tubo-ovarian abscess
- In all patients: Mesenteric lymphadenitis (enlarged right iliac fossa nodes with a normal appendix and terminal ileum thickening), terminal ileitis (Crohn's disease, Yersinia, Campylobacter), cecal diverticulitis, omental infarction
- In older patients: Cecal carcinoma causing secondary appendiceal obstruction must be excluded — an irregular cecal mass with appendiceal distension warrants urgent attention. Mucocele of the appendix is another important consideration
Pediatric Considerations: Radiation Minimization
In pediatric patients, radiation dose minimization is a primary ethical obligation. Ultrasound is recommended as the first-line imaging modality for suspected appendicitis in children due to its radiation-free nature and sensitivity of 80–92% when the appendix is visualized by an experienced sonographer. CT is reserved for cases where ultrasound is indeterminate or technically limited. When CT is performed in children, low-dose protocols with exclusively IV contrast and targeted scanning of the abdomen and pelvis are standard of care, typically yielding an effective dose of less than 3 mSv.
Standardized CT Reporting for Appendicitis
A high-quality CT report for suspected appendicitis should systematically address: the visualization status of the appendix (identified vs. not seen vs. collapsed/normal); appendiceal outer diameter measurement; presence or absence of an appendicolith; description of periappendiceal inflammatory changes (fat stranding, local free fluid, free gas); assessment for complications (gangrene, perforation, abscess formation); and consideration of alternative diagnoses when the appendix appears normal. The conclusion should provide a clear, unambiguous diagnostic statement — either confirming appendicitis, excluding it, or suggesting the most likely alternative diagnosis — to guide timely and appropriate clinical management.